WARFARIN
(i) Tujuan/ Kegunaan Ubat
Warfarin digunakan untuk menghalang pembentukan darah beku dan
menghalang darah beku sedia ada daripada menjadi semakin besar. Ia
kerap dipreskripsikan untuk pesakit yang mengalami degupan jantung tak
sekata tertentu dan/atau bagi mereka yang telah melalui serangan jantung
atau pembedahan penggantian injap jantung. Warfarin berfungsi dengan
menghentikan pembentukan bahan yang menyebabkan darah beku serta
mencegah berlakunya trombosi dan embolism.
(ii) Cara Penggunaan
Administrasi
Ikut arahan pada label pengubatan. Makan tablet pada masa yang sama
sekali sehari. Terdapat jenama warfarin yang berbeza (contohnya,
Marevan®, APO-Wafarin®).
Jangan tukar jenama kerana ia mungkin mempunyai keberkesanan yang
berbeza.
Jika terlupa
Ambil dos yang tertinggal sebaik sahaja anda teringat, jika ianya dalam
tempoh hari yang sama. Teruskan mengambil warfarin anda pada waktu
yang sama pada keesokan hari. Jangan gandakan dos. Menggandakan
dos mungkin menyebabkan peningkatan pendarahan. Catatkan tarikh dos
yang tertinggal dan beritahu doktor anda semasa janji temu anda yang
seterusnya.
Penyimpanan
Jauhi dari kelembapan (simpan di tempat yang kering) dan kepanasan
(elakkan daripada sinaran terus matahari)
Simpan ubat di tempat yang selamat dan jauh daripada kanak-kanak
Peringatan
Kehamilan: Warfarin boleh menyebabkan kecacatan semasa lahir.
Maklumkan doktor atau ahli farmasi anda jika anda hamil atau berhasrat
untuk hamil.
Pembedahan: Jika anda akan melalui pembedahan (termasuk
pembedahan gigi) maklumkan doktor atau doktor gigi berkenaan bahawa
anda mengambil warfarin. Doktor mungkin meminta anda berhenti
mengambil warfarin selama beberapa hari sebelum prosedur tersebut
untuk mengelakkan pendarahan berlebihan.
Alkohol: Elakkan pengambilan alkohol berlebihan. Dinasihatkan supaya
tidak mengambil lebih daripada 5 tin bir atau lebih daripada 1 botol wain
seminggu.
Aktiviti Harian: Berhati-hati apabila menggunakan pisau cukur dan objek
tajam lain. Elakkan sukan lasak (contohnya, bola sepak, rugbi, seni
mempertahankan diri) atau aktiviti yang boleh mencederakan anda
.Elakkan penggunaan berus gigi, floss yang keras.
Kecederaan: Sekiranya anda mengalami kecederaan ringan, basuh dan
berikan tekanan atas kawasan tersebut sehingga pendarahan berhenti (ini
mungkin mengambil masa sehingga 10 minit). Dapatkan perhatian
perubatan dengan segera jika pendarahan banyak berlaku pada tempat
cedera atau jika anda mengalami kecederaan di kepala. Teruskan
memberi tekanan pada tempat luka sambil menunggu bantuan.
Peringatan:
Semasa anda mengambil warfarin, anda perlu kembali untuk
pemeriksaan darah secara berkala. Pada setiap temu janji dengan doktor
anda, pemeriksaan darah akan diarahkan untuk memeriksa Nisbah
Ternormal Antarabangsa (INR), yang mencerminkan keberkesanan
rawatan antikoagulasi. Jadi, penting bagi anda menghadiri setiap temu janji
untuk memastikan bahawa warfarin diberikan dengan wajar. Sentiasa buat
janji temu lain jika anda gagal menghadiri salah satu. Anda hendaklah
pertimbangkan membawa kad pengenalan (Buku Panduan untuk Pesakit
Warfarin) untuk menunjukkan yang anda mengambil warfarin. Ini penting
terutamanya semasa kecemasan atau apabila anda tidak sedar. Berunding
dengan ahli farmasi atau doktor anda mengenai cara mendapatkan kad ini.
(iii) Interaksi
Drug – Drug
Banyak pengubatan mengganggu keberkesanan warfarin. Penting bagi
anda memberitahu doktor atau ahli farmasi anda jika anda mengambil
pengubatan lain termasuk pengubatan tanpa preskripsi, tradisional dan
herba. Ini termasuk:
o Antasid
o Batuk atau ubat selesema
o Ubat ulser gaster
o Julap
o Ubat tahan sakit (contohnya, aspirin dan NSAIDS lain)
o Vitamin tambahan (Vitamin
K)
Drug – Makanan
Bincang diet anda dengan doktor. Jangan lakukan sebarang perubahan
besar terhadap pengambilan makanan yang mengandungi vitamin K,
seperti hati, sayuran berdaun hijau dan brokoli, kerana ia mungkin
mengubah kesan warfarin.
Drug- Herba
Dinasihatkan supaya tidak mengambil apa-apa Jamu, ubat Cina (Gingko
Biloba, Ginseng, Dong Quai) atau Ayurvedik , kerana kesannya terhadap
warfarin tidak boleh diramal.
(iv) Kesan Ubat
Kesan Terapeutik
Mencegah dan merawat darah beku di dalam saluran darah.
Kesan Sampingan
Kesan sampingan clopidogrel yang paling biasa ialah pendarahan.
Lebam-lebam: Anda mungkin mudah menjadi lebam sekiranya jatuh atau
terlanggar sesuatu. JANGAN gosok atau urut kawasan tersebut. Sila
dapatkan perhatian perubatan jika lebam bertambah besar atau saiznya
tidak berkurangan, atau jika anda mendapat lebam-lebam tanpa sebab
nyata.
Pendarahan: Sila dapatkan perhatian pengamal perubatan sekiranya anda
mengalami simptom berikut
:
o Pendarahan daripada telinga, hidung, gusi (jangan lupa
menggunakan berus gigi lembut)
o Muntah darah (yang mungkin kelihatan seperti serbuk kopi atau
darah segar)
o Sakit perut tanpa sebab
o Bintik merah pada kulit
o Kesakitan atau pembengkakan luar biasa (con. Pada sendi)
o Darah dalam air kencing
o Darah haid yang banyak
o Pendarahan rektum
o Najis hitam, melekit
Friday, March 27, 2015
Saturday, March 14, 2015
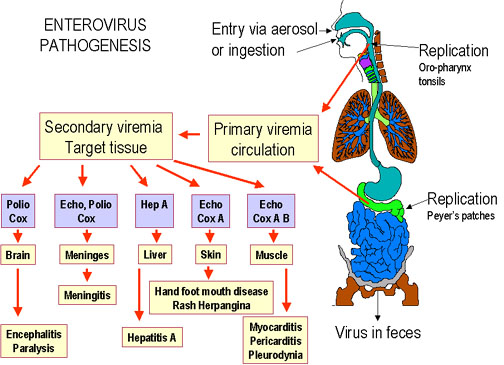
COXSAKIEVIRUS HAND-FOOT-MOUTH DISEASE
What is hand-foot-and-mouth disease?
Hand-foot-and-mouth disease (HFMD) is a common illness of infants and children.
SYMPTOMS
- Fever, sores in the mouth, and a rash with blisters.
- Begins with a mild fever, poor appetite, malaise, and a sore throat.
- One or two days after the fever begins, sores develop in the mouth. They begin as small red spots that blister and then often become ulcers. They are usually located on the tongue, gums, and inside of the cheeks.
- The skin rash develops over one to two days with flat or raised red spots, some with blisters. The rash does not itch, and it is usually located on the palms of the hands and soles of the feet. It may also appear on the buttocks.
- A person with HFMD may have only the rash or the mouth ulcers.

Is HFMD the same as foot-and-mouth disease?
No. HFMD is a different disease from foot-and-mouth disease of cattle, sheep, and swine. Although the names are similar, the two diseases are not related at all and are caused by different viruses.
Is HFMD serious?
Usually not. Nearly all people with HFMD recover without medical treatment. HFMD usually resolves in seven to ten days. There are no common complications. Rarely, this illness may be associated with aseptic or viral meningitis, in which the person has fever, headache, stiff neck, or back pain, and may need to be hospitalized for a few days.
What causes HFMD?
Several different viruses cause HFMD. The most common cause is coxsackievirus A16; occasionally, other strains of coxsackievirus A or enterovirus 71 cause HFMD. The coxsackieviruses are members of a group of viruses called the enteroviruses. The enterovirus group includes polioviruses, coxsackieviruses, and echoviruses.
Is it contagious?
Yes, HFMD is moderately contagious. Infection is spread from person to person by direct contact with nose and throat discharges or the stool of infected persons. A person is most contagious during the first week of the illness. HFMD is not transmitted to or from pets or other animals.
How soon will someone become ill after getting infected?
The usual period from infection to onset of symptoms is three to six days. Fever is often the first symptom of HFMD.
Who is at risk for HFMD?
HFMD occurs mainly in children under 10 years old, but adults may also be at risk. Everyone is susceptible to infection. Infection results in immunity to the specific virus, but a second episode may occur following infection with a different one of the enteroviruses.
When and where does HFMD occur?
Individual cases and outbreaks of HFMD occur worldwide, more frequently in summer and early autumn.



Diuretics
DIURETICS
INDUCE DIURESIS -- > INCREASE URINE VOLUME
Classification
DRUGS CLASSIFICATION
1. Acetic Anhydrase Inhibitor (AAI)
eg. ACETAZOLAMIDE
- weak diuretics.
- Act on PCT (proximal convoluted tubule).
- it increases NAHCO3 excretion, making your urine alkaline & salty.
- INCREASE NA/H20 EXCRETION.
Mnemonics ''GUMA''
Mnemonics ''ACID MANS''
- hypercholemia metabolic acidosis
- neuropathy (due to increase seizure threshold)
- ammonia toxicity (ammonia reabsorption -->hepatic encephalopathy)
- sulfa allergy (renal damage, crystalluria, rash, blood dysrasia)
But if you’re allergic to sulfur, then you better adjust your doses. Don’t take too much since it could cause hyperchloremic metabolic acidosis.
2. OSMOTIC DIURETICS:
it targets your PCT, makes you pee, and increases fluid osmolarity.
Mnemonic ''GUM''
MANNITOL
Uses: '' BCGS''
B- Barturate Poisoning
C- Cerebral Edema
G- Glaucoma
S- Stroke /Shock
C/I : ''CAP'
*** If you have CHF or Anuria, DON’T take mannitol if you know whats good for ya!
3. THIAZIDE DIURETICS
Hydrochlorothiazides
Chlorothiazides
Thiazide diuretics use (4) MNEMONIC ''HE IS DOCTOR'' - DOC FIRST IN HTN^^
SE of thiazide diuretics (4)
HyperGLUC

4. LOOP DIURETICS
What is different about ethcyrnic acid compared to the other loop diuretics ???(important)
it is not a sulfonamide thus it can be used when a pt has a sulfa allergy
If you are allergic to sulfur yet edematous & want to live, take ethacrynic acid instead cause its a phenoxyacetic acid derivative.
Loop diuretics use (3)
O -ototoxicity
H- hypokalemia
D- dehydration
A - sulfa allergy
N -nephritis (interstitial)
G- gout
D/I
Mnemonics ''L and D''
L = Lithium - decreased clearance
A = Aminoglycosides ( due to ototoxicity)
D = Digitalis (due to hypokalemia)
5. POTASSIUM SPARING DIURETICS
2 different MoA (depends on locations)
- Disted Convoluted Tubule (DCT) --> Triamterene, Amiloride .
INDUCE DIURESIS -- > INCREASE URINE VOLUME
Classification
- Acetic anhydride inhibitor
- Osmotic Diuretics
- Potassium sparing diuretics
- Loop diuretics
- Thiazides
DRUGS CLASSIFICATION
1. Acetic Anhydrase Inhibitor (AAI)
eg. ACETAZOLAMIDE
- weak diuretics.
- Act on PCT (proximal convoluted tubule).
- it increases NAHCO3 excretion, making your urine alkaline & salty.
- INCREASE NA/H20 EXCRETION.
“ACID”azolamide causes ACIDosis.USES
Mnemonics ''GUMA''
- Glaucoma
- Urinary alkalizer
- Metabolic alkalosis
- Prophylaxis of mountain sickness
Mnemonics ''ACID MANS''
- hypercholemia metabolic acidosis
- neuropathy (due to increase seizure threshold)
- ammonia toxicity (ammonia reabsorption -->hepatic encephalopathy)
- sulfa allergy (renal damage, crystalluria, rash, blood dysrasia)
But if you’re allergic to sulfur, then you better adjust your doses. Don’t take too much since it could cause hyperchloremic metabolic acidosis.
2. OSMOTIC DIURETICS:
it targets your PCT, makes you pee, and increases fluid osmolarity.
Mnemonic ''GUM''
- Glycerol
- Urea
- Mannitol
MANNITOL
Uses: '' BCGS''
B- Barturate Poisoning
C- Cerebral Edema
G- Glaucoma
S- Stroke /Shock
C/I : ''CAP'
- If cerebral hemorrphage --> C/I ( as Mannitol can escape from hemorrphagic vessels & cause dehydration of brain cells via osmotic action)
- Pulmonary edema
- anuria ???
- CHF (it causes tachycardia)
*** If you have CHF or Anuria, DON’T take mannitol if you know whats good for ya!
3. THIAZIDE DIURETICS
Hydrochlorothiazides
Chlorothiazides
THIAZIDE - 1ST DOC for HYPERTENSION.
- MoA - Act on DCT (distal convoluted tubules).
- Increase Na, K, Cl, H20 excretion.
- Increase Calcium reabsorption.
Thiazide diuretics use (4) MNEMONIC ''HE IS DOCTOR'' - DOC FIRST IN HTN^^
- HTN
- CHF
- idiopathic hypercalcuria
- nephrogenic diabetes insipidus
- Generalised Edema
SE of thiazide diuretics (4)
HyperGLUC
- glycemia
- lipidemia
- uricemia
- calcemia
4. LOOP DIURETICS
- ethacrynic acid
- furosemide
- bumetanide
- torsemide
What is different about ethcyrnic acid compared to the other loop diuretics ???(important)
it is not a sulfonamide thus it can be used when a pt has a sulfa allergy
If you are allergic to sulfur yet edematous & want to live, take ethacrynic acid instead cause its a phenoxyacetic acid derivative.
Loop diuretics use (3)
- Edema (CHF, cirrhosis, nephrotic syndrome)
- HTN
- hypercalcemia
O -ototoxicity
H- hypokalemia
D- dehydration
A - sulfa allergy
N -nephritis (interstitial)
G- gout
D/I
Mnemonics ''L and D''
L = Lithium - decreased clearance
A = Aminoglycosides ( due to ototoxicity)
D = Digitalis (due to hypokalemia)
5. POTASSIUM SPARING DIURETICS
increase excretion of Na, Cl, H20 but RETAIN POTASSIUM K.
(mnemonic) K+ STAys
Spironolactone
triamterene
amiloride
Spironolactone
triamterene
amiloride
2 different MoA (depends on locations)
- Disted Convoluted Tubule (DCT) --> Triamterene, Amiloride .
-Collecting Tubule(CT) --> spironolactone
Treatment
SE (2)
Treatment
- - hypertension often combination with thiazide diuretics or loop diuretics.
- - hypoaldosteronism.
SE (2)
- hyperaldosteronism
- hyperkalemia
- gynecomastia (via an antiandrogen effect)
ACE INHIBITORS
ACE INHIBITORS
''Angiotensin converting enzyme'' inhibitorS
Mnemonics
ALL end with -APRIL.
Police Lazy Come Record For Entertain (6)
P - Perindopril
L -Lisinopril
C - Captopril
R -Ramipril
F -Fosinoapril
E - Enalapril
ACE-I
MoA
-Block the enzyme ACE that catalyse conversion of Angiotensin I to angiotensin II ; thus cause vasodilatation --> decrease peripheral resistance --> reduce afterload --> reduce DBP. --> in turn reduce preload & SBP --> reduce blood pressure.
-by reducing production of angiotensin II, ACE inhibitors allow blood vessels to widen, which lowers blood pressure and improves heart output.

Two mains clinical APPS of ACE-I
1. Vasodilatation
2. Reduce platelet aggregation
USES OF ACE-I
1. Heart
- Hypertension
- Congestive heart failure
- Myocardial infarction
- Prophylaxis of cardiovascular risk
2, Diabetic Neuropathy
3. Scleroderma renal crisis - deterioration of renal function & marked rise of BP.
ACE-I
Suitable for:
1. Young patients
2. Left ventricular hypertrophy
3, Gout
4. PVD - peripheral vascular disease
'5. dyslipidemic patients

ContraindicationS
Hyperkalemia
Pregnancy
Renal artery stenosis
Preexisting dry cough ( batuk tanpa kahak) due to increased bradykinin level

''Angiotensin converting enzyme'' inhibitorS
Mnemonics
ALL end with -APRIL.
Police Lazy Come Record For Entertain (6)
P - Perindopril
L -Lisinopril
C - Captopril
R -Ramipril
F -Fosinoapril
E - Enalapril
ACE-I
MoA
-Block the enzyme ACE that catalyse conversion of Angiotensin I to angiotensin II ; thus cause vasodilatation --> decrease peripheral resistance --> reduce afterload --> reduce DBP. --> in turn reduce preload & SBP --> reduce blood pressure.
-by reducing production of angiotensin II, ACE inhibitors allow blood vessels to widen, which lowers blood pressure and improves heart output.

Two mains clinical APPS of ACE-I
1. Vasodilatation
2. Reduce platelet aggregation
1. Heart
- Hypertension
- Congestive heart failure
- Myocardial infarction
- Prophylaxis of cardiovascular risk
2, Diabetic Neuropathy
3. Scleroderma renal crisis - deterioration of renal function & marked rise of BP.
ACE-I
Suitable for:
1. Young patients
2. Left ventricular hypertrophy
3, Gout
4. PVD - peripheral vascular disease
'5. dyslipidemic patients
ContraindicationS
Hyperkalemia
Pregnancy
Renal artery stenosis
Preexisting dry cough ( batuk tanpa kahak) due to increased bradykinin level

Tuesday, March 10, 2015
Calcium Channel Blockers (CCBs)
Calcium channel Blockers
Mnemonics
''VERY NICE DRUGS''
V - Verapamil
N - Nifedipine
D - Diltiazem
CCBs can be subdivided according to structural and functional distinctions.
1. Dihydropyridine:
Mnemonic FAN
F- felodipine
A - amlodipine,
N - nicardipine, nifedipine, nisoldipine
2. Phenylalkylamine : verapamil
3. Benzothiazepine: diltiazem
Calcium & muscle contraction
voltage gated calcium channel (VGCC) located in the cells that undergo depolarisation eg muscles, glial cell, neurone--> lead to muscle contraction.
calcium is stored in the sarcoplasmic reticulum,
Tropomyosin is coiled around the actin filament by the help of another protein known as troponin.
in the other words, troponin we said it is attached to tropomyosin.
Tropomyosin functions to prevent myosin from binding to the actin filament.
To unblock it( allow myosin attached to actin filament) --> troponin need change its shape and conformation.
How troponin can change its shape? Good questions??
When calcium ion present in high conc., calcium ion will bind to troponin and move the tropomyosin ''out of way'' and push actin filament to the right side.
once the calcium ion bound to troponin & troponin change its shape, the myosin able to bind to actin filament and finally lead to muscle contraction.
after sometimes, calcium ions become lesser. Low conc of calcium get released from troponin. Troponin then goes back to its original shape, make tropomyosin block myosin again.
MoA
- Prevent calcium ion ( for muscle contraction) from entering into smooth and cardiac muscle cells.
- thus, it lower systolic & diastolic BP --> reduce angina.
- Some CCBs eg. Procaine( nifedipine) slow electrical impulse that run through heart muscle, it helps to regulate arrhythmia.
clinical apps of CCB
''CHASMA''
C - Congestive Heart Failure
H - HTN
A-Angina
S- Supreventricular tachyarrthymias
M- Migraine (same as beta blockers)
A- Atrial flutter / atrial fibrillation
IMPORTANT = CCBs is DOC for atrial flutter/ atrial fibrillation.
CAUTIONS
Caution should be taken when using verapamil with a beta blocker due to the risk of severe bradycardia.
Mnemonics
''VERY NICE DRUGS''
V - Verapamil
N - Nifedipine
D - Diltiazem
CCBs can be subdivided according to structural and functional distinctions.
1. Dihydropyridine:
Mnemonic FAN
F- felodipine
A - amlodipine,
N - nicardipine, nifedipine, nisoldipine
2. Phenylalkylamine : verapamil
3. Benzothiazepine: diltiazem
Calcium & muscle contraction
voltage gated calcium channel (VGCC) located in the cells that undergo depolarisation eg muscles, glial cell, neurone--> lead to muscle contraction.
calcium is stored in the sarcoplasmic reticulum,
Tropomyosin is coiled around the actin filament by the help of another protein known as troponin.
in the other words, troponin we said it is attached to tropomyosin.
Tropomyosin functions to prevent myosin from binding to the actin filament.
To unblock it( allow myosin attached to actin filament) --> troponin need change its shape and conformation.
How troponin can change its shape? Good questions??
When calcium ion present in high conc., calcium ion will bind to troponin and move the tropomyosin ''out of way'' and push actin filament to the right side.
once the calcium ion bound to troponin & troponin change its shape, the myosin able to bind to actin filament and finally lead to muscle contraction.
after sometimes, calcium ions become lesser. Low conc of calcium get released from troponin. Troponin then goes back to its original shape, make tropomyosin block myosin again.
MoA
- Prevent calcium ion ( for muscle contraction) from entering into smooth and cardiac muscle cells.
- thus, it lower systolic & diastolic BP --> reduce angina.
- Some CCBs eg. Procaine( nifedipine) slow electrical impulse that run through heart muscle, it helps to regulate arrhythmia.
clinical apps of CCB
''CHASMA''
C - Congestive Heart Failure
H - HTN
A-Angina
S- Supreventricular tachyarrthymias
M- Migraine (same as beta blockers)
A- Atrial flutter / atrial fibrillation
IMPORTANT = CCBs is DOC for atrial flutter/ atrial fibrillation.
CAUTIONS
Caution should be taken when using verapamil with a beta blocker due to the risk of severe bradycardia.
Monday, March 9, 2015
beta blocker
beta blockers


why we said our blood pressure will increase after exercise or when we're getting nervous?
this is because when we get nervous, our body sympathetic nerves system will secrete hormones epinephrine/ norepinephrines (which both comes under catecholamine category) into bloodstream.

These two hormones will travel in bloodstream and target on the beta 1- adrenergic receptor which is located in heart. This receptor stimulation will in turn cause:
1. positive inotropic = increase force of contraction
2. positive chronotropic = increase heart rate
3. increase cardiac conduction velocity and automaticity
 Not only heart, beta 2 receptor also located in kidney.
Not only heart, beta 2 receptor also located in kidney.
Epinephrine and norephinephrine hormone will stimulate release of renin in the kidney.
Renin will catalyse the conversion of angiotensiongen--> angiotension I; and then angiotension II.
In the end, it will cause vasoconstriction --> lead to rise in BP.
SUMMARY
Beta 1 receptor stimulation --> cardiac stimulation and lipolysis
Beta 2 receptor stimulation --> bronchodilation and blood vessels relaxation (usually skeletal muscles)

 ***Cardioselective beta blockers will act on beta 1 receptor BUT its selectivity will be LOST in high dose.
***Cardioselective beta blockers will act on beta 1 receptor BUT its selectivity will be LOST in high dose.
Beta Blockers
1. Cardioselective B1 blockers
end with -LOL
"Betablockers Acting Exclusively At Myocardium"
B - BetaxoLOL
E - EsmoLOL
A - AtenoLOL
M -MetaproLOL
Beta-blockers: nonselective beta-blockers "Tim Pinches His Nasal Problem" (because he has a runny nose...):
Timolol
Pindolol
Hismolol
Naldolol
Propranolol
Beta blockers: B1 selective vs. B1-B2 non-selective A through N: B1 selective: Acebutalol, Atenolol, Esmolol, Metoprolol.
Clinical apps of beta blockers
1. ANGINA
2. ARRHYTHMIA
3. HYPERTENSION
other considerations
1, Contraindicated in ASTHMATIC patients.
- as beta blocker impair the relaxation of bronchial smooth muscles.
- when beta receptor stimulated --> activate SNS --> heart contract and beat more --> BP increases.
- At the same time, bronchial smooth muscles also get relaxed so that more oxygen in the lungs can be diffused into bloodstream to compensate the oxygen demand in out body.
2. Topical-->Treat glaucoma --> decrease intraocular pressure by decrease aqueous humor secretion. But it can diffuse into blood stream and cause systemic effects.
3. Since they lower HR and reduce tremor, used by Olympics marksmen to enhance performance BUT banned.

![]()




why we said our blood pressure will increase after exercise or when we're getting nervous?
this is because when we get nervous, our body sympathetic nerves system will secrete hormones epinephrine/ norepinephrines (which both comes under catecholamine category) into bloodstream.

These two hormones will travel in bloodstream and target on the beta 1- adrenergic receptor which is located in heart. This receptor stimulation will in turn cause:
1. positive inotropic = increase force of contraction
2. positive chronotropic = increase heart rate
3. increase cardiac conduction velocity and automaticity

Epinephrine and norephinephrine hormone will stimulate release of renin in the kidney.
Renin will catalyse the conversion of angiotensiongen--> angiotension I; and then angiotension II.
In the end, it will cause vasoconstriction --> lead to rise in BP.
SUMMARY
Beta 1 receptor stimulation --> cardiac stimulation and lipolysis
Beta 2 receptor stimulation --> bronchodilation and blood vessels relaxation (usually skeletal muscles)


Beta Blockers
1. Cardioselective B1 blockers
end with -LOL
"Betablockers Acting Exclusively At Myocardium"
ABEAM
A - AcebuteLOLB - BetaxoLOL
E - EsmoLOL
A - AtenoLOL
M -MetaproLOL
Beta-blockers: nonselective beta-blockers "Tim Pinches His Nasal Problem" (because he has a runny nose...):
Timolol
Pindolol
Hismolol
Naldolol
Propranolol
Beta blockers: B1 selective vs. B1-B2 non-selective A through N: B1 selective: Acebutalol, Atenolol, Esmolol, Metoprolol.
O through Z: B1, B2 non-selective: Pindolol, Propanalol, Timolol.
Clinical apps of beta blockers
1. ANGINA
2. ARRHYTHMIA
3. HYPERTENSION
other considerations
1, Contraindicated in ASTHMATIC patients.
- as beta blocker impair the relaxation of bronchial smooth muscles.
- when beta receptor stimulated --> activate SNS --> heart contract and beat more --> BP increases.
- At the same time, bronchial smooth muscles also get relaxed so that more oxygen in the lungs can be diffused into bloodstream to compensate the oxygen demand in out body.
2. Topical-->Treat glaucoma --> decrease intraocular pressure by decrease aqueous humor secretion. But it can diffuse into blood stream and cause systemic effects.
3. Since they lower HR and reduce tremor, used by Olympics marksmen to enhance performance BUT banned.
Beta-blockers: main contraindications, cautions
ABCDE:
Asthma
Block (heart block)
COPD
Diabetes mellitus
Electrolyte (hyperkalemia)
Sunday, March 8, 2015
Angina Pectoralis 心绞痛
ANGINA PECTORALIS
- chest pain with exertion
- 3 types:
a. stable angina - chest pain with exertion, Relieved with Rest. It can predictable.
- Provoked by 3 E:
E = Eating
E = Emotion
E = Exercise
b. unstable angina - chest pain with exertion, DO NOT Relieved with Rest
- Need TREAT IMMEDIATELY.
c. Prinztmetal / Variant angina - chest pain in cycle( occurs same time every day); may occur during rest. Due to vasospasm of coronary artery (due to smooth muscle of vessel wall contraction rather than reason of atherosclerosis plaque) --> lead to narrowing of coronary artery.
-In other words, means that PA can happen in the person without history of atherosclerosis,
- It's NOT predictable.
-Its more associate with SAD.
S = Smoking
A = Alcohol
D= Drug Abuse
- Calcium channel Blocker (CCB) is DOC for the vasospasm of C.A.
Causes of AP
- result from heart require more oxygen from available.
- DEMAND > SUPPLY
- Eg. during exercise or work up, a person exerted more works and need more oxygen than supplied, results in lack of oxygen supplied to heart, and consequently lead to myocardium ischemia(lack of oxygen). ---> chest pain arises.
- Its also means coronary artery diseases.
- Refer to formation of atherosclerosis plaque (high rich in cholesterol) in the coronary artery( artery that responsible in delivering oxygen to hearts) ---> narrowing of coronary artery ---> decreases blood and oxygen delivered to heart --> heart receives no adequate oxygen and thus chest pain occurs.
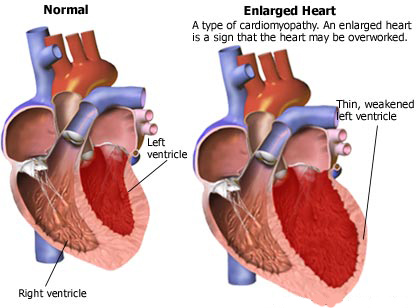
- Sometimes, a heart artery is completed blocked by a plaque or clots. When this occurs, the blood flow to heart STOPS. Without blood, the cells of affected heart muscles will permanently damaged. That called HEART ATTACK.


Symptoms
- severe chest pain, may radiate to the arms, shoulder, back of body, jaws and necks.
- some even feel indigestion or nausea or vomiting,
- feeling of tightness or heaviness in arms, elbow, and wrists. (mainly in left sides)
- fatigue and shortness of breath,
- symptoms usually occurs when a person exerts lots of physical efforts for few minutes. it goes away when person takes rest or take medications. Sometimes, it may occur during rest.

The signs of heart attack is quite similar to angina pectoralis.
So, How we gonna differentiate both?
there are three main differentiation:
1. the duration longer > 5 minutes,
2. Pain of heart attack is more severe.
3. Medications and rest do not relieve its pain.
However, if left untreated, angina may also lead to heart attack. Initiate treatment immediately once confirmed angina occurs.
Diagnosis??
The doctor may do several tests. An Electrocardiogram (ECG)is used to record heart rhythm.
A stress ECG may be done. during the test, the patient is asked to exercise on the treadmill or bicycle while an ECG is taken. Change in ECG pattern will help doctor to diagnose coronary artery disease.
An ECG is pain free and has no complications.
Complications are rare during stress ECG. if any problems, immediate treatment must be available.
Patient who cannot exercise will be given medication to make heart beat work faster. This medication helps to stimulate exercising.
an Echocardiogram is another test to measure heart structure and function. the doctor analyses its heart function image on the screen. Typically painless.
another test is called nuclear scan is used to study heart function. a small amount of radioactive material is injected into vein, and a camera will take picture of heart. the part of heart that do not getting enough oxygen will be showed up in the picture.

- chest pain with exertion
- 3 types:
a. stable angina - chest pain with exertion, Relieved with Rest. It can predictable.
- Provoked by 3 E:
E = Eating
E = Emotion
E = Exercise
b. unstable angina - chest pain with exertion, DO NOT Relieved with Rest
- Need TREAT IMMEDIATELY.
c. Prinztmetal / Variant angina - chest pain in cycle( occurs same time every day); may occur during rest. Due to vasospasm of coronary artery (due to smooth muscle of vessel wall contraction rather than reason of atherosclerosis plaque) --> lead to narrowing of coronary artery.
-In other words, means that PA can happen in the person without history of atherosclerosis,
- It's NOT predictable.
-Its more associate with SAD.
S = Smoking
A = Alcohol
D= Drug Abuse
- Calcium channel Blocker (CCB) is DOC for the vasospasm of C.A.
Causes of AP
- result from heart require more oxygen from available.
- DEMAND > SUPPLY
- Eg. during exercise or work up, a person exerted more works and need more oxygen than supplied, results in lack of oxygen supplied to heart, and consequently lead to myocardium ischemia(lack of oxygen). ---> chest pain arises.
- Its also means coronary artery diseases.
- Refer to formation of atherosclerosis plaque (high rich in cholesterol) in the coronary artery( artery that responsible in delivering oxygen to hearts) ---> narrowing of coronary artery ---> decreases blood and oxygen delivered to heart --> heart receives no adequate oxygen and thus chest pain occurs.
- Sometimes, a heart artery is completed blocked by a plaque or clots. When this occurs, the blood flow to heart STOPS. Without blood, the cells of affected heart muscles will permanently damaged. That called HEART ATTACK.

Symptoms
- severe chest pain, may radiate to the arms, shoulder, back of body, jaws and necks.
- some even feel indigestion or nausea or vomiting,
- feeling of tightness or heaviness in arms, elbow, and wrists. (mainly in left sides)
- fatigue and shortness of breath,
- symptoms usually occurs when a person exerts lots of physical efforts for few minutes. it goes away when person takes rest or take medications. Sometimes, it may occur during rest.
The signs of heart attack is quite similar to angina pectoralis.
So, How we gonna differentiate both?
there are three main differentiation:
1. the duration longer > 5 minutes,
2. Pain of heart attack is more severe.
3. Medications and rest do not relieve its pain.
However, if left untreated, angina may also lead to heart attack. Initiate treatment immediately once confirmed angina occurs.
Diagnosis??
The doctor may do several tests. An Electrocardiogram (ECG)is used to record heart rhythm.
A stress ECG may be done. during the test, the patient is asked to exercise on the treadmill or bicycle while an ECG is taken. Change in ECG pattern will help doctor to diagnose coronary artery disease.
An ECG is pain free and has no complications.
Complications are rare during stress ECG. if any problems, immediate treatment must be available.
Patient who cannot exercise will be given medication to make heart beat work faster. This medication helps to stimulate exercising.
an Echocardiogram is another test to measure heart structure and function. the doctor analyses its heart function image on the screen. Typically painless.
another test is called nuclear scan is used to study heart function. a small amount of radioactive material is injected into vein, and a camera will take picture of heart. the part of heart that do not getting enough oxygen will be showed up in the picture.

Angina Mnemonics
Angina
Management through lifestyle alterations
Mnemonic: SLEW
S Smoking cessation
L Low-fat diet
E Exercise
W Weight loss
Management of acute unstable angina
Mnemonic: 2 As and BALI
A Admit, bed rest, high-flow oxygen
A Analgesia
A Aspirin and clopidogrel
B Beta blockers
A Angiography with or without angioplasty/CABG if symptoms fail to improve
L Low molecular weight heparin (LMWH)
I Infusion of nitrates
Management through lifestyle alterations
Mnemonic: SLEW
S Smoking cessation
L Low-fat diet
E Exercise
W Weight loss
Management of acute unstable angina
Mnemonic: 2 As and BALI
A Admit, bed rest, high-flow oxygen
A Analgesia
A Aspirin and clopidogrel
B Beta blockers
A Angiography with or without angioplasty/CABG if symptoms fail to improve
L Low molecular weight heparin (LMWH)
I Infusion of nitrates
Subscribe to:
Posts (Atom)